
Metastasis Is Not Spread — It’s the Body Building More Storage Vaults
In my theory of cancer, we can understand metastasis as the body’s intelligent attempt to contain an overwhelming toxic load.

Welcome to my blog! If you’re new here, let me explain that we are rewriting the theory of cancer, one blog post at a time. The puzzle pieces all seem to fall together once we accept that cancer tumors are built intentionally by the body, as a key defense against toxic overload. I call this the Toxin Sequestration Theory (TST) of cancer, where the job of cancer tumors is to sequester, store, and process toxins that would otherwise damage the body’s tissues and organs.
One of the most common questions I get about TST is how can it explain metastasis - the process whereby cancer spreads from one organ to another. Indeed, nothing strikes more fear into the heart of a cancer patient than the word “metastasis.” The moment doctors mention that the cancer has spread, the conversation shifts from “Can we remove it?” to “How long do I have?” This is unfortunate, and I believe that my blog post will offer a more hopeful view on metastasis.
Mainstream medicine typically describes metastasis as the disease becoming more aggressive — rogue cells breaking free, invading distant organs, and colonizing the body. It is portrayed as the tumor turning malicious, as if the cancer has suddenly decided to go on the offensive. But what if metastasis is not the cancer becoming more evil… but the body running out of safe storage space?
In TST, a tumor is not a rogue growth. It is an emergency storage vault — a secondary detox organ the body builds when the liver, kidneys, and lungs can no longer handle the toxic load. The tumor sequesters harmful substances (seed oils, excess iron, oxalate, ammonia, microplastics, and many others) to protect the rest of the body.
Metastasis, then, is not a sign of defeat. It is what happens when that first vault becomes overwhelmed. When the toxic burden continues to rise and the primary tumor can no longer contain it all, the body is forced to create additional sequestration sites in distant organs. The cancer spreads not because it wants to kill the host, but because the body is desperately trying to keep the toxins isolated and away from vital, delicate tissues. This single reframing changes everything about how we understand metastasis — and what we should do about it.
Why The Mainstream View Falls Short
Mainstream oncology describes metastasis as a hallmark of cancer’s aggressiveness. Cancer cells are said to acquire new mutations that allow them to detach from the primary tumor, survive in the bloodstream or lymphatics, and successfully colonize distant organs. This process is portrayed as the disease progressing to a more dangerous, almost intentional phase — the tumor “learning” how to spread and conquer the body.
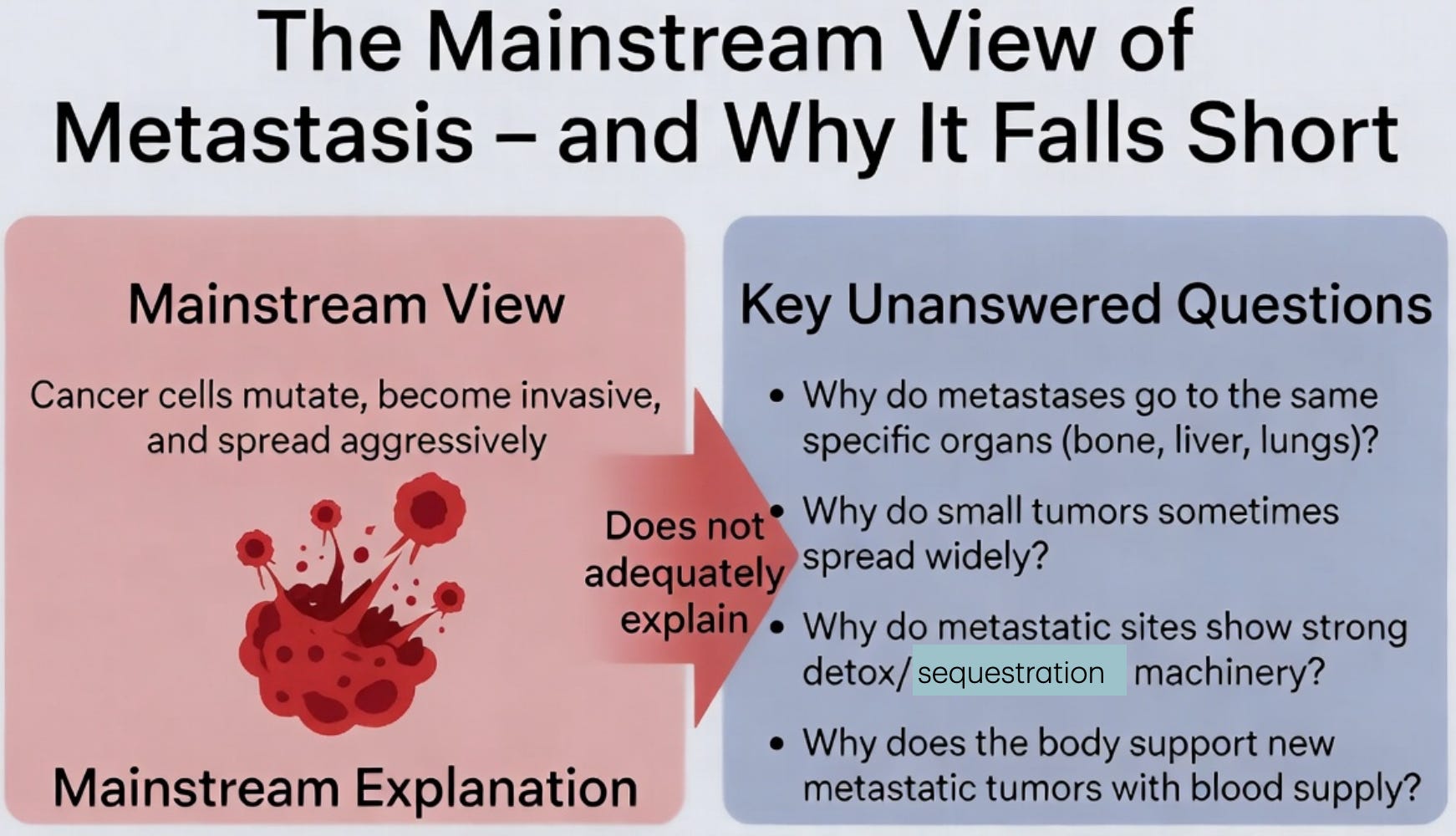
This explanation leaves several critical observations poorly explained:
Why do metastases so often appear in predictable organs (bones, liver, and lungs) rather than randomly?
Why do some patients with very small primary tumors develop widespread metastases, while others with large tumors do not?
Why do metastatic sites sometimes show even higher expression of the same detox and sequestration machinery (GLUT transporters, CD36, ferritin, etc.) seen in the primary tumor?
Why does the body seem to “cooperate” in the process by providing blood supply (angiogenesis) and stromal support to the new metastatic lesions?
The last objection is especially powerful, as our bodies would not just provide help unwittingly to a foreign entity trying to conquer it.
From the perspective of Toxin Sequestration Theory, these patterns make far more sense when viewed through a different lens. Metastasis is not the cancer cells becoming more vicious. It is the body creating secondary emergency storage vaults when the primary tumor can no longer handle the toxic load on its own.
Metastasis as Secondary Sequestration Sites
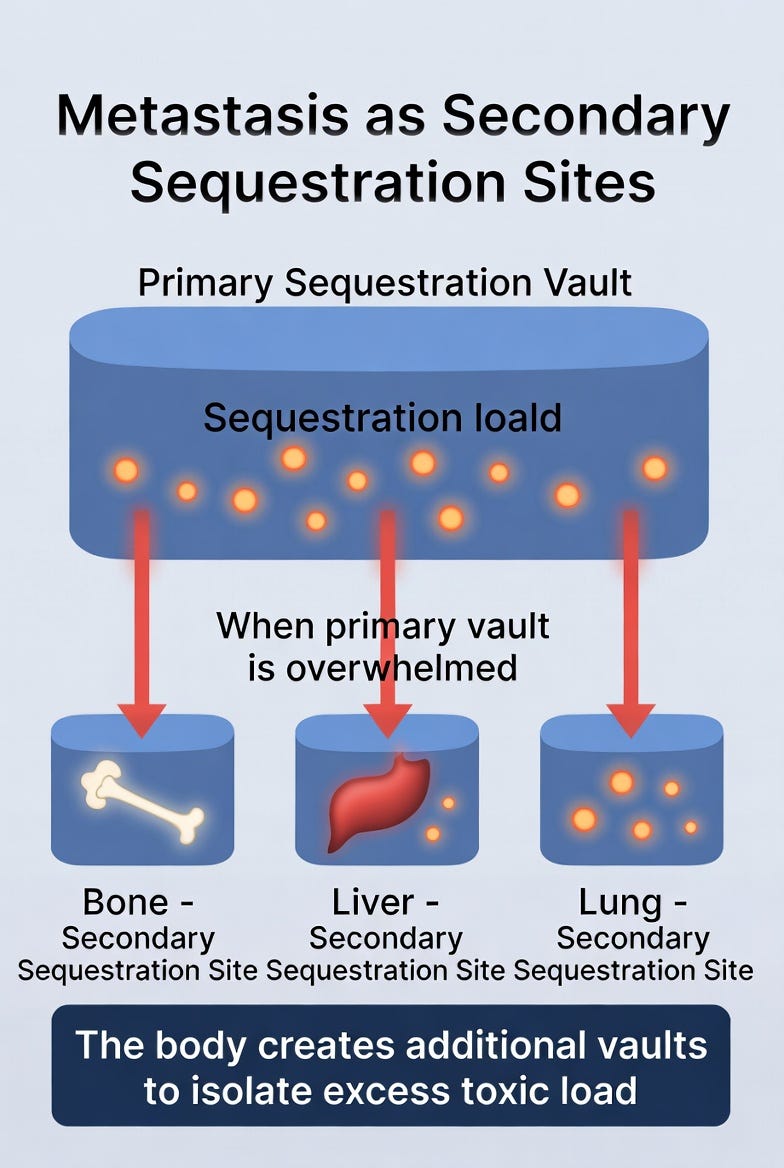
In Toxin Sequestration Theory, metastasis is not a sign that cancer has become more aggressive or malicious. It is the body’s attempt to build secondary emergency storage vaults when the primary tumor can no longer contain the toxic load on its own.
When the influx of toxins (fructose, heavy metals, deuterium, ethanol, or other redox stressors) exceeds the capacity of the first sequestration site, the body faces a difficult choice: allow systemic toxicity to rise dangerously, or create additional compartments to isolate the excess burden. Metastasis is the body choosing the latter.
This explains several otherwise puzzling patterns:
Metastases frequently appear in organs that are either heavily burdened by a specific toxin (e.g., bone for iron, liver for various xenobiotics, lungs for airborne or lipid-soluble toxins) or capable of providing high-capacity storage with relatively less immediate risk to survival.
Metastatic tumors often show even higher expression of sequestration machinery — upregulated GLUT transporters, CD36 for fatty acids, ferritin for iron, and other detox enzymes — than the primary tumor.
The body frequently supports the new metastatic sites with robust blood supply and stromal tissue, as if it is deliberately investing in the new storage facility.
Far from being a random or purely destructive process, metastasis represents the body’s continued effort to protect vital organs by distributing the toxic overload across multiple sequestration sites. The cancer is still functioning as a protective response — just one that has been forced to scale up because the original vault is overflowing.
Why Do Cancer Cells Migrate?
Mainstream oncology describes metastasis as a process in which cancer cells detach from the primary tumor, enter the bloodstream or lymphatic system as circulating tumor cells, survive the journey, and establish colonies in distant organs. Substantial evidence supports this dissemination model, including the detection of genetically matched tumor cells in the blood and in secondary sites.
Toxin Sequestration Theory does not dispute that cells migrate. It simply offers a very different explanation for why the body uses this mechanism.
Imagine the primary tumor as the body’s first emergency sequestration vault, already working at full capacity to contain a rising flood of toxins and redox stress. At some point the vault reaches its limit. The body now faces an urgent crisis: it must create additional high-capacity storage sites quickly, or risk systemic toxicity overwhelming vital organs.
Rather than slowly building entirely new tumors from scratch in distant tissues, the body chooses a far more efficient strategy. It dispatches specialized cells (or small clusters of cells) from the existing, battle-tested primary vault. These migrating cells are not rogue invaders — they are pre-adapted construction crews. They already carry everything needed to begin effective sequestration the moment they arrive: upregulated GLUT transporters, high ferritin levels, robust redox-handling machinery, and the metabolic adaptations required to tolerate intense oxidative stress.
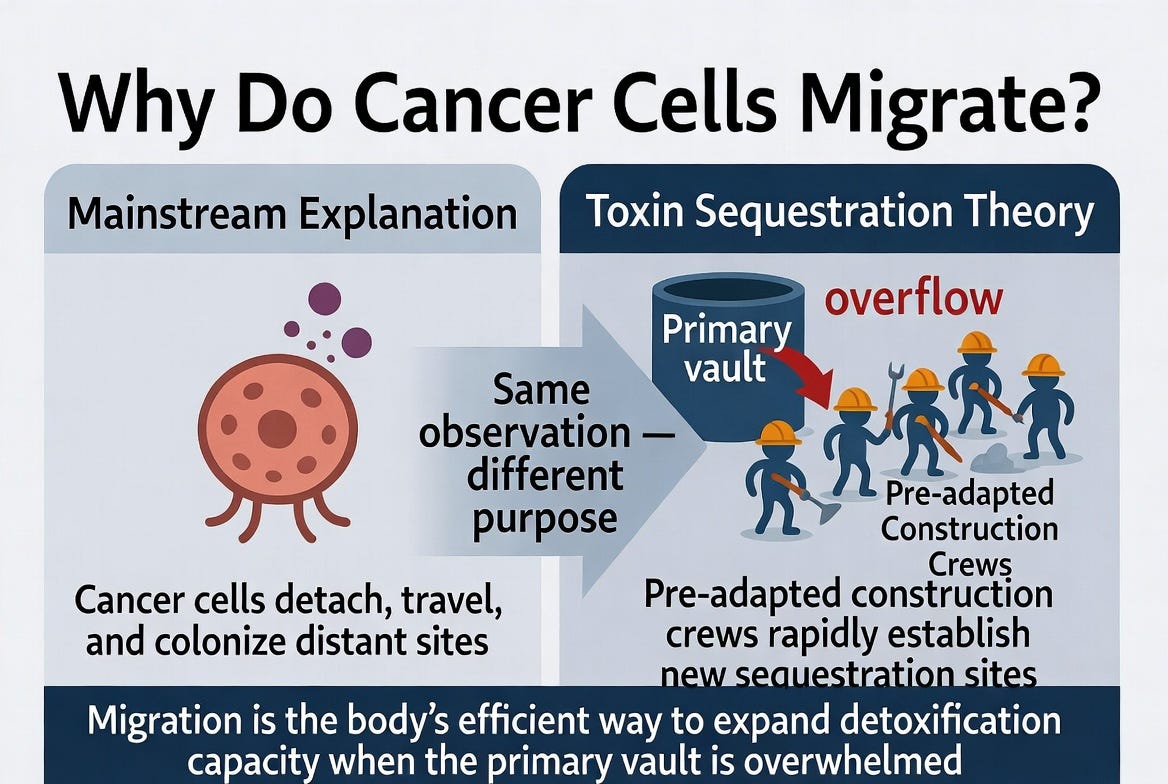
By sending these ready-made teams ahead, the body can rapidly establish new, fully functional storage vaults exactly where they are needed most. Migration, therefore, is not an act of conquest. It is a sophisticated, coordinated logistical response — the body’s intelligent way of scaling up its detoxification capacity when the original vault can no longer keep pace with the toxic load.
Evidence for Pre-Adapted Construction Crews
This idea is not mere speculation. Modern cancer research has repeatedly shown that the cells most successful at forming metastases are not random — they are pre-adapted subpopulations already equipped with the necessary traits while still inside the primary tumor.
Studies have identified small groups of cells within primary tumors that already express high levels of GLUT transporters, elevated ferritin, altered redox-handling metabolism, and other sequestration-related machinery long before they disseminate. These “metastasis-initiating cells” or “pre-metastatic” clones are significantly more likely to survive the journey through the blood and successfully establish new tumors in distant organs. Genetic tracking experiments confirm that many metastatic lesions are seeded by these pre-existing, better-equipped subpopulations rather than by average cells from the primary tumor.
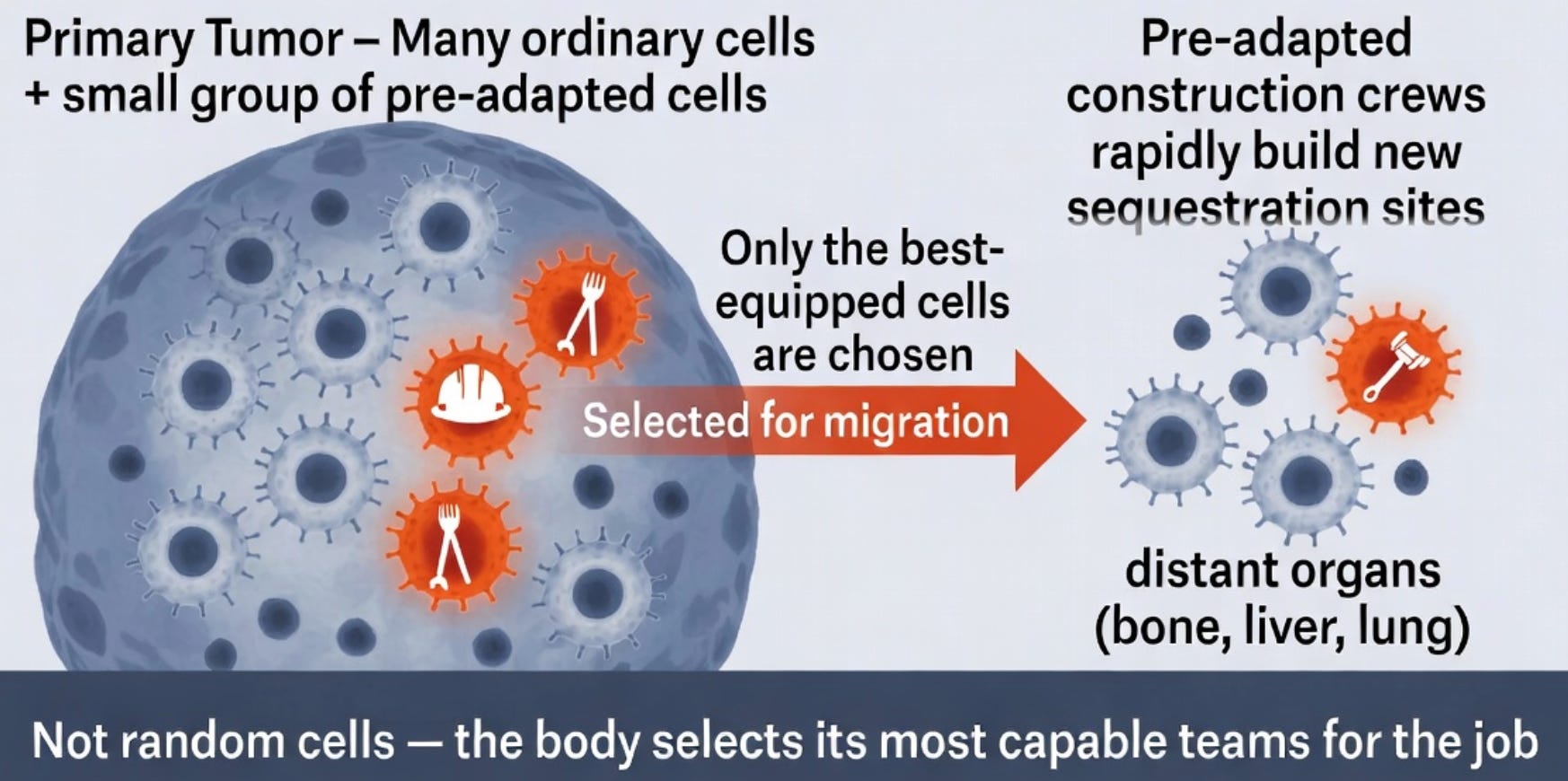
In TST terms, the body is not sending out generic cells and hoping for the best. It is strategically deploying its most experienced and best-equipped “construction crews” — cells that have already proven they can handle high toxic loads — to rapidly build new, fully functional sequestration vaults when the primary site becomes overwhelmed. This pre-adaptation explains why metastasis can occur relatively quickly and efficiently once the toxic burden exceeds the capacity of the first vault.
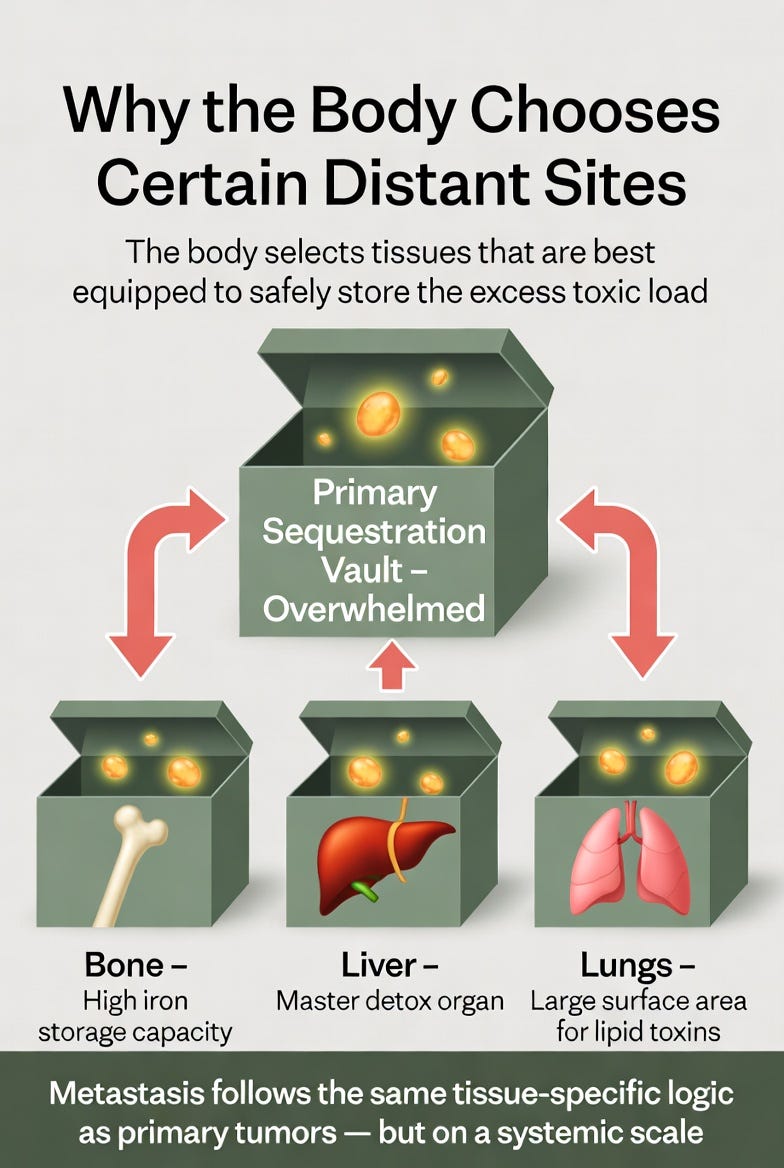
Why the Body Chooses Certain Distant Sites
If metastasis is the body building additional sequestration vaults, why do new tumors so often appear in predictable locations — bones, liver, lungs, brain, or lymph nodes?
The answer lies in the same principle that governs primary tumor location discussed in my previous post about Tissue-Specific Toxin Sequestration Theory (TSTST). Namely, the body selects tissues that are either most heavily burdened by the specific toxins or best equipped to safely isolate and store them without immediately threatening survival.
Just as the primary tumor forms in the organ best suited to handle the dominant toxic load (prostate for seed oils and hormones, breast for excess estrogen, liver for alcohol and xenobiotics), metastatic sites follow the same logic on a systemic scale:
Bone is frequently chosen when iron overload or heavy metal burden is high — bone marrow has enormous storage capacity and natural affinity for iron sequestration.
Liver becomes a common secondary site because it is already the body’s master detox organ and has robust machinery for handling a wide range of toxins.
Lungs are often targeted for lipid-soluble or airborne-derived toxins, as they provide large surface area and high blood flow for rapid sequestration.
Brain is a last-resort site, used only when toxins are particularly neurotoxic or when the body has run out of safer options.
The body does not scatter metastases randomly. It strategically expands its sequestration network to tissues that can absorb the overflow most effectively. This is the same tissue-specific logic you saw in primary tumors, now operating on a larger, multi-site scale. Metastasis is therefore not chaotic invasion. It is the body’s intelligent, last-ditch effort to distribute an unmanageable toxic burden across multiple specialized storage compartments.
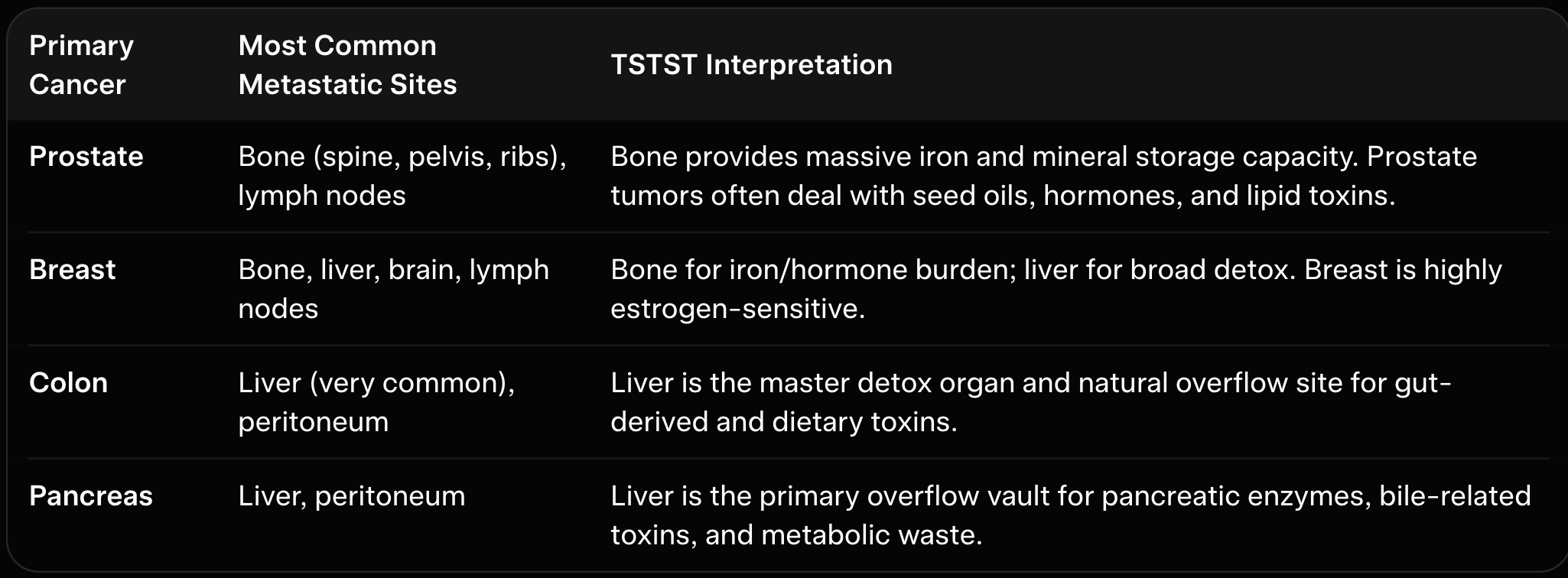
The table above shows that certain primary tumors give rise to specific metastatic sites. These patterns are not random. In TST, the body continues to follow the same tissue-specific logic it used when forming the primary tumor. It strategically selects secondary sites that are either already heavily burdened by the dominant toxins or best equipped to safely store and isolate the excess load. Bone and liver appear frequently because they offer large storage capacity with relatively lower immediate risk to survival. Metastasis, therefore, represents a calculated expansion of the body’s detoxification infrastructure when the original vault becomes overwhelmed.
Specific Toxins → Specific Metastatic Sites
Toxin Sequestration Theory predicts that the type of toxic burden influences where secondary vaults are built. The body doesn’t choose metastatic sites randomly — it chooses them based on which tissues are best equipped to handle the dominant toxins overflowing from the primary tumor.
Excess iron or heavy metals → strong preference for bone (especially spine and pelvis), because bone marrow has enormous iron storage capacity.
Hormonal toxins / excess estrogen → common spread to bone and liver, tissues that can help manage hormone-related oxidative stress.
Lipid-soluble toxins and oxidized seed oils → frequent metastasis to liver and lungs, organs with high capacity for handling fats and lipids.
Gut-derived and dietary toxins (common in colon and pancreatic cancers) → heavy preference for the liver, the body’s master detox organ.
These patterns are not coincidences. They reflect the body’s intelligent attempt to distribute the toxic load to the tissues most capable of safely sequestering it. In this sense, the location of metastases gives us clues about which toxins are overwhelming the system.
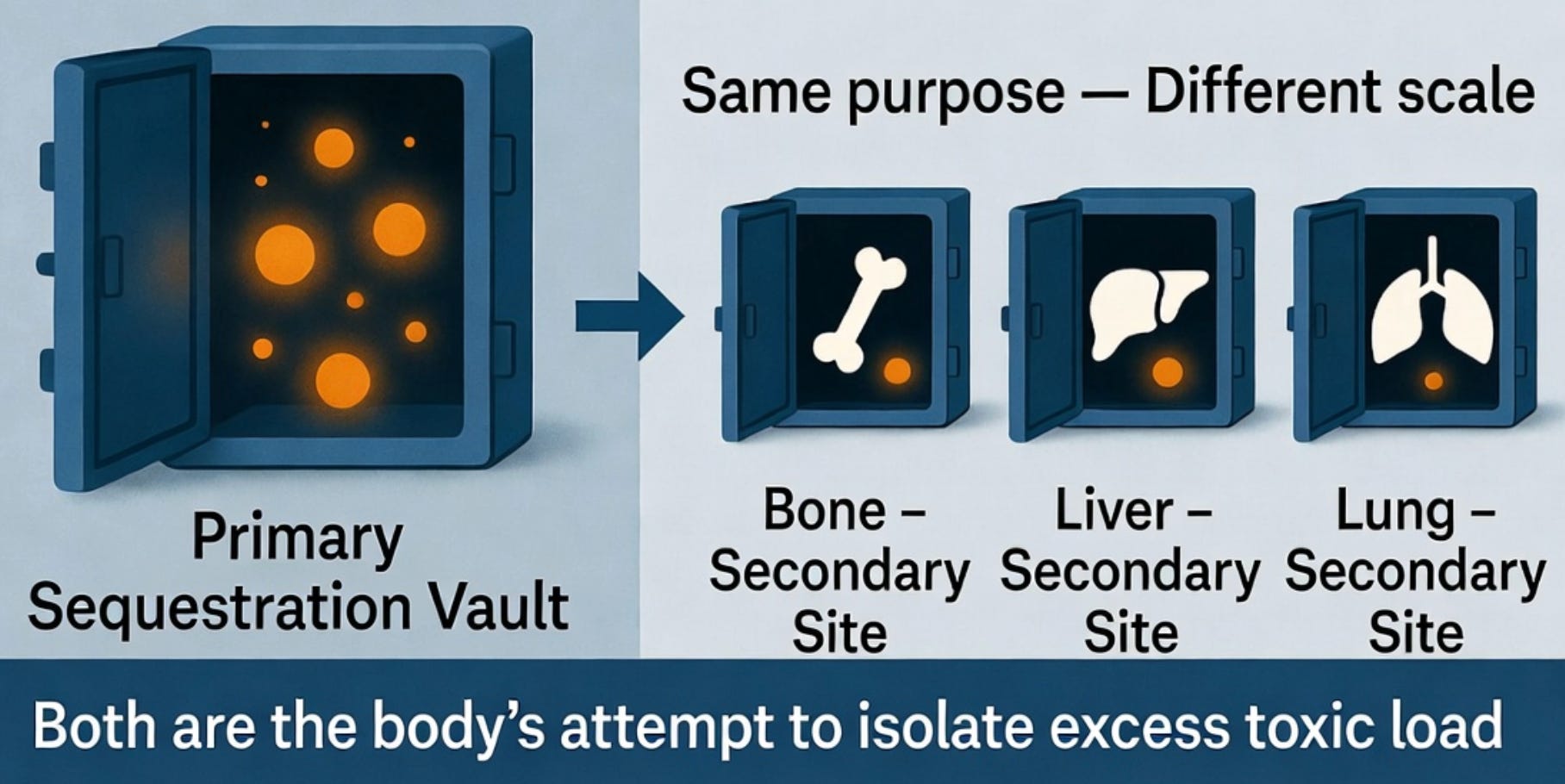
Primary Tumor vs Metastatic Tumors: Same Purpose, Different Scale
In Toxin Sequestration Theory, there is no fundamental difference in purpose between the primary tumor and its metastases.
The primary tumor is the body’s first emergency sequestration vault — built when the liver and other primary detox systems could no longer handle the toxic load.
When that first vault reaches capacity, the body does not give up. It simply scales up the same strategy. Metastatic tumors are secondary sequestration vaults created for exactly the same reason: to isolate and store excess toxins that the original site can no longer safely contain.
Both the primary tumor and its metastases express similar sequestration machinery — upregulated transporters for glucose, lipids, and metals; elevated ferritin for iron storage; and altered metabolism designed to tolerate high oxidative stress. They are performing the same job, just at different locations and scales.
The appearance of metastases does not mean the body has lost control. It means the toxic burden has grown so large that one vault is no longer enough. The body is responding exactly as it was designed to: by expanding its emergency storage infrastructure to protect the rest of the organism.
TST Resolves the Failures of the Mainstream View
Mainstream oncology struggles to explain several consistent and puzzling features of metastasis. Why do metastases so reliably appear in the same handful of organs — bone, liver, lungs, and sometimes brain — rather than appearing randomly across the body? Why do small primary tumors sometimes produce widespread metastases while large ones remain localized? And why does the body often provide robust blood supply and stromal support to the new metastatic sites, as if it is actively helping them grow?
Toxin Sequestration Theory resolves these observations elegantly. Metastasis is not random cellular rebellion. It is the body deliberately expanding its sequestration network when the primary vault becomes overwhelmed. The body chooses specific distant sites for the same reason it chose the location of the primary tumor: those tissues are either already heavily burdened by the dominant toxins or best equipped to safely store and isolate the excess load.
Bone is frequently selected because of its massive iron and mineral storage capacity. The liver is chosen as the master detox organ capable of handling a broad range of toxins. The lungs provide large surface area and high blood flow for lipid-soluble or volatile toxins. The predictable organ preference is therefore not mysterious — it is the logical outcome of the body’s attempt to distribute an unmanageable toxic burden as efficiently and safely as possible.
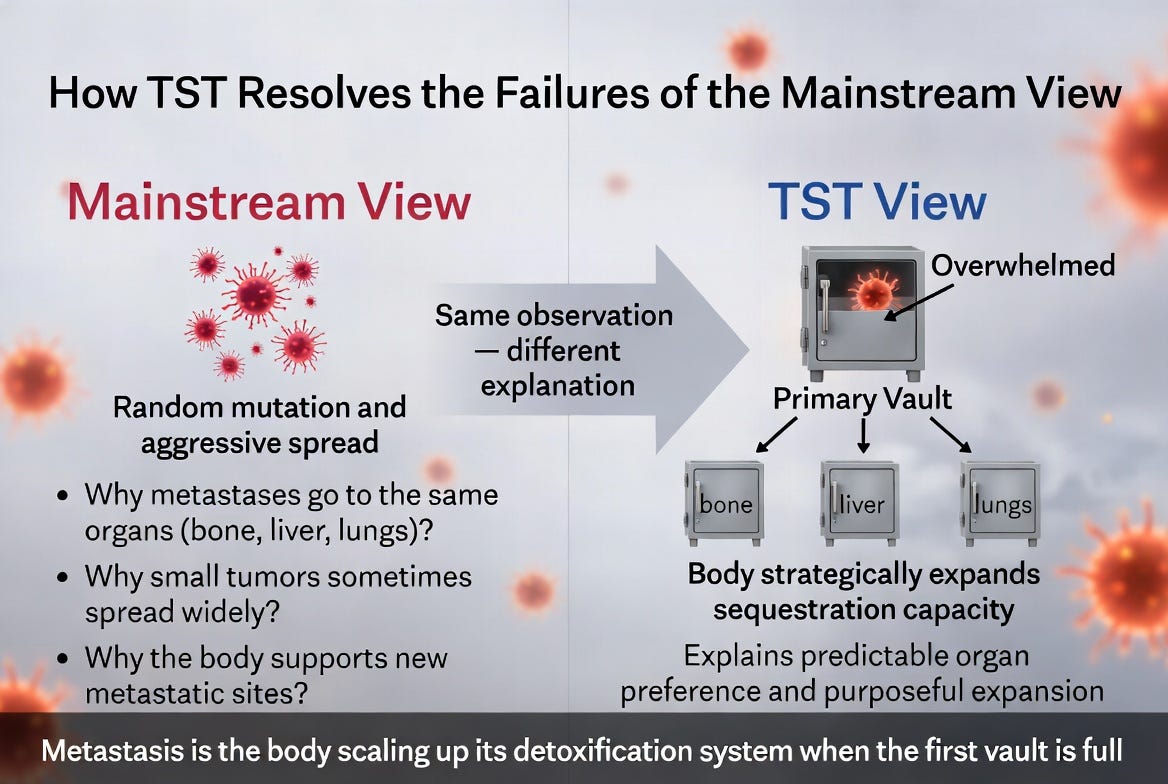
By reframing metastasis as a protective scaling-up of sequestration capacity rather than random aggression, TST explains patterns that the mutation-driven model has long left unexplained.
Implications for Treatment and Prognosis
If metastasis is the body’s attempt to expand its detoxification capacity when the primary sequestration vault becomes overwhelmed, then our entire approach to treatment needs rethinking.
Conventional therapies often focus on aggressively attacking both the primary tumor and its metastases with chemotherapy, radiation, or surgery — essentially trying to destroy the very vaults the body has built to contain toxins. While these treatments may shrink tumors in the short term, they can also release stored toxins back into circulation and further damage the body’s already strained detox systems. This may explain why many patients experience rapid decline after aggressive treatment of metastatic disease.
From the perspective of TST, a more rational strategy would be to reduce the underlying toxic load that created the need for these vaults in the first place. When the influx of toxins decreases and the liver and primary detox organs regain capacity, the pressure on both the primary tumor and its metastases should ease. The body may then no longer need to maintain these emergency storage sites, allowing natural regression or stabilization to occur.
This does not mean ignoring tumors entirely. It means shifting the primary goal from “killing every cancer cell” to “lightening the toxic burden so the body no longer requires such extensive sequestration infrastructure.” In some cases, supporting the body’s own resolution mechanisms may prove more effective — and far less damaging — than trying to eradicate every secondary site.
What This Means for Hope and Healing
Understanding metastasis through TST changes the emotional weight of the diagnosis. The appearance of new tumors is no longer proof that the body has lost control or that the cancer is “winning.” It is evidence that the body is still fighting — still trying to protect vital organs by creating additional storage vaults when the first one is full.
This perspective offers real hope. If the driving force behind metastasis is excess toxic load, then the patient can take real, tangible actions to address the root cause. The priority becomes reducing the underlying toxic burden so the body no longer needs such extensive sequestration infrastructure. When the influx of toxins decreases and the liver and primary detox systems regain capacity, the pressure on both the primary tumor and its metastases often eases. In some cases, tumors stabilize or even regress as the body no longer requires them as emergency storage sites.
Metastasis is not necessarily a death sentence. It may simply be a sign that the body needs more help managing its toxic load.
Conclusion
In summary, this blog tried to take the intense fear out of metastasis, reinterpreting it not as malicious spread of cancer but rather as the body adding new storage vaults for toxins. Strikingly, the body appears to choose specific organs for metastases - bones, liver, and lungs - as these organs are best equipped to handle additional toxic load. It’s difficult for the mainstream theory to explain why these same organs repeatedly appear in metastases. Hence, TST offers deeper insight into metastasis than the mainstream view.
Thanks for reading! Let me know your thoughts!
I completely agree. The toxic load is the problem.
Great article.... makes perfect sense. The body is designed to survive..... God's temple, God's design, no mistakes